Alcohol Use Disorder (AUD) is a chronic, relapsing brain disorder characterized by an impaired ability to stop or control alcohol use despite adverse social, occupational, or health consequences. According to the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-5), AUD is classified into three severity levels: mild, moderate, and severe, based on how many of 11 diagnostic criteria a person meets. The National Institute on Alcohol Abuse and Alcoholism (NIAAA) estimates that approximately 29.5 million Americans aged 12 and older had AUD in 2021, making it one of the most prevalent substance use disorders worldwide.
Recognizing the signs and symptoms of AUD is critical because early identification significantly improves treatment outcomes. Symptoms span three domains: physical signs such as tremors and chronic facial flushing, psychological signs such as intense cravings and emotional dysregulation, and behavioral signs such as hiding drinking habits or prioritizing alcohol over personal responsibilities. Many individuals dismiss early warning signs as normal social drinking, which delays intervention and allows the disorder to progress to more severe stages.
The causes of AUD are multifactorial, involving a complex interaction of genetic predisposition, neurochemical imbalances, psychological vulnerability, and social environment. The effects are equally wide-ranging, damaging the liver, brain, heart, personal relationships, and professional life over time. Fortunately, evidence-based treatment options exist, including medically supervised detoxification, pharmacotherapy, cognitive behavioral therapy, and peer support programs. Understanding each of these dimensions fully equips individuals, families, and clinicians to respond effectively and compassionately to this condition.
What Is Alcohol Use Disorder?
Alcohol Use Disorder is a chronic brain disease defined by compulsive alcohol consumption, loss of control over the amount consumed, and a negative emotional state when alcohol is not available, meeting at least 2 of 11 DSM-5 criteria within a 12-month period.
To understand AUD more precisely, it helps to examine how it is formally defined, how it differs from ordinary heavy drinking, and how severity is stratified clinically.
Definition According to DSM-5
AUD is formally defined by the American Psychiatric Association in DSM-5 as a problematic pattern of alcohol use leading to clinically significant impairment or distress. Specifically, a clinician diagnoses AUD when a patient meets 2 or more of 11 standardized criteria within any 12-month window. These criteria include inability to cut down despite wanting to, spending excessive time obtaining or recovering from alcohol, craving, neglecting responsibilities, continued use despite relationship problems, tolerance, and withdrawal.
The shift from DSM-IV to DSM-5 was clinically significant: the older edition separated “alcohol abuse” and “alcohol dependence” into two distinct diagnoses, while DSM-5 merged them into a single spectrum disorder. This change better reflects the biological continuum of the condition and reduces the stigma associated with the word “dependence.” Meeting 2 to 3 criteria indicates mild AUD, 4 to 5 indicates moderate AUD, and 6 or more indicates severe AUD.
According to the World Health Organization (WHO, 2022), harmful use of alcohol accounts for approximately 3 million deaths per year globally, representing 5.3% of all deaths, underscoring the clinical and public health urgency of accurate AUD definition and diagnosis.
How AUD Differs from Heavy Drinking or Binge Drinking
AUD is not the same as heavy drinking or binge drinking, though either pattern can escalate into AUD over time. Heavy drinking is defined by the NIAAA as consuming more than 4 drinks on any day or more than 14 drinks per week for men, and more than 3 drinks on any day or more than 7 per week for women. Binge drinking refers to a pattern that brings blood alcohol concentration to 0.08% or higher, typically occurring when a man drinks 5 or more drinks, or a woman drinks 4 or more drinks, within about 2 hours.
The critical distinction is that AUD involves a loss of control and a compulsive quality to drinking that persists even when the person clearly wants to stop and even when drinking is causing real harm. Heavy drinking is a behavior; AUD is a disorder of the brain’s reward, stress, and executive control circuits. Importantly, not all heavy drinkers develop AUD, but chronic heavy drinking is the most significant behavioral risk factor for its development.
What Are the Signs and Symptoms of Alcohol Use Disorder?
There are three main categories of AUD symptoms: physical symptoms such as tremors and coordination loss, psychological symptoms such as cravings and anxiety when not drinking, and behavioral symptoms such as secretive drinking and neglecting obligations.
Correctly identifying these symptoms, particularly in their early stages, is essential for timely intervention. The following sections detail early warning signs and the physical manifestations that emerge as the disorder progresses.
What Are the Early Warning Signs of Alcohol Use Disorder?
The earliest warning signs of AUD are a gradual increase in alcohol tolerance, relying on alcohol to relax or sleep, and feeling uncomfortable or irritable in social situations without drinking. These signs are frequently misattributed to stress or personality, which is why AUD is often diagnosed years after onset.
Specifically, early warning signs include:
- Drinking more than intended on most occasions: A person plans to have one or two drinks but consistently consumes four or five.
- Increased tolerance: Needing noticeably more alcohol to achieve the same effect that fewer drinks once produced.
- Using alcohol as emotional regulation: Reaching for a drink specifically to manage stress, anxiety, loneliness, or boredom rather than for social enjoyment.
- Preoccupation with drinking occasions: Frequently thinking about the next opportunity to drink or planning activities around alcohol availability.
- Mild withdrawal discomfort: Experiencing slight shakiness, irritability, or difficulty concentrating the morning after drinking, which resolves quickly with another drink.
- Minimizing or hiding consumption: Downplaying how much one drinks to family members or drinking secretly before social events.
A key clinical distinction between social drinking and early AUD is the element of compulsion and the emerging inability to consistently stop at a self-determined limit. According to a longitudinal study published in JAMA Psychiatry (Grant et al., 2017), over 72% of adults in the United States will meet the criteria for AUD at some point in their lifetime when using DSM-5 criteria, and a significant proportion first exhibit symptoms in early adulthood without recognizing them as clinically relevant.
What Are the Physical Symptoms of Alcohol Use Disorder?
The physical symptoms of AUD become increasingly pronounced as the disorder progresses from mild to severe, affecting the liver, nervous system, cardiovascular system, and gastrointestinal tract. Early physical signs include persistent facial redness (due to vasodilation), disrupted sleep architecture, and reduced motor coordination. As AUD advances, more serious physical manifestations emerge:
- Liver damage indicators: Jaundice (yellowing of skin and eyes), abdominal swelling from ascites, and right upper quadrant pain signal hepatic involvement ranging from fatty liver disease to cirrhosis.
- Neurological signs: Peripheral neuropathy causing numbness or tingling in hands and feet, poor balance and coordination (ataxia), and involuntary hand tremors, especially noticeable in the morning.
- Cardiovascular effects: Elevated blood pressure, irregular heartbeat (arrhythmia), and cardiomyopathy (weakening of the heart muscle) in chronic heavy drinkers.
- Gastrointestinal symptoms: Chronic gastritis, pancreatitis causing severe abdominal pain, and esophageal varices (enlarged veins that can rupture).
- Hormonal disruption: In men, chronic alcohol use suppresses testosterone, leading to reduced libido, muscle loss, and gynecomastia. In women, it disrupts menstrual cycles and accelerates bone density loss.
According to the American Liver Foundation (2023), alcohol-related liver disease accounts for nearly 50% of all liver cirrhosis deaths in the United States, and most patients with alcohol-induced cirrhosis have been consuming alcohol heavily for 10 or more years before the diagnosis.
What Are the Causes of Alcohol Use Disorder?
The causes of Alcohol Use Disorder fall into three broad categories: biological factors including genetics and neurochemistry, psychological factors including trauma and co-occurring mental health conditions, and social or environmental factors including peer influence and family dynamics.
No single cause produces AUD. Instead, the disorder emerges from a convergence of multiple risk factors that interact over time. The following sections examine the genetic and psychological contributors in greater depth.
Is Alcohol Use Disorder Genetic?
Yes, AUD has a significant genetic component, with heritability estimated at approximately 50 to 60%, meaning that genetic factors account for roughly half of a person’s risk of developing the disorder. Children of parents with AUD are 4 times more likely to develop the condition themselves, even when raised in different environments.
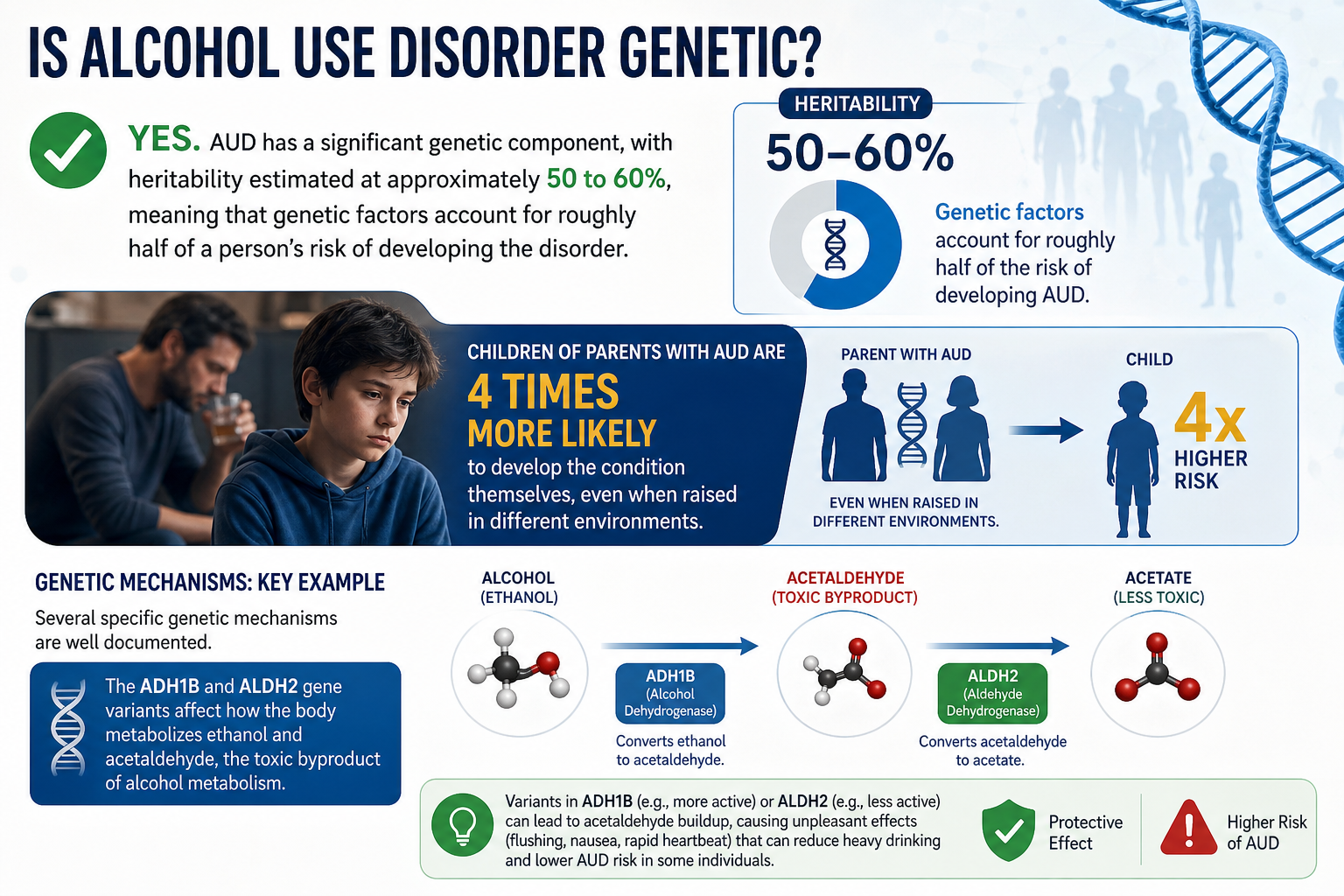
Several specific genetic mechanisms are well documented. The ADH1B and ALDH2 gene variants affect how the body metabolizes ethanol and acetaldehyde, the toxic byproduct of alcohol breakdown. Individuals with certain ALDH2 variants experience flushing, nausea, and rapid heartbeat when drinking, which acts as a natural deterrent. Conversely, genetic variants that promote faster conversion of ethanol to acetaldehyde and slower clearance increase the subjective reward of drinking and reduce negative physical feedback.
Beyond metabolism genes, research has identified genetic variants in dopaminergic, serotonergic, and GABA receptor systems that influence reward sensitivity and impulse control. The DRD2 gene, which encodes the dopamine D2 receptor, has been associated with reduced receptor density in people with AUD, reducing the brain’s natural reward response and increasing the likelihood of seeking artificial stimulation through alcohol.
According to a twin study published in Psychological Medicine by Kendler et al. (2011), genetic influences on AUD are largely shared with genetic risk for other substance use disorders, suggesting a common underlying biological predisposition rather than alcohol-specific genetics.
Can Mental Health Conditions Cause Alcohol Use Disorder?
Yes, mental health conditions can significantly contribute to the development of AUD through a mechanism known as self-medication, where individuals use alcohol to reduce the distress of untreated anxiety, depression, post-traumatic stress disorder (PTSD), or other psychiatric conditions. This relationship is bidirectional: mental illness increases AUD risk, and AUD worsens mental illness outcomes.
The self-medication hypothesis, first formalized by Khantzian (1985) and extensively supported by subsequent research, proposes that people gravitate toward specific substances based on their psychopharmacological effects. Alcohol, as a central nervous system depressant that enhances GABA activity and reduces cortisol release, provides temporary relief from anxiety and hyperarousal symptoms associated with PTSD and generalized anxiety disorder.
This co-occurrence is so common that clinicians use the term “dual diagnosis” or “comorbidity” to describe patients presenting with both AUD and a psychiatric condition. Key statistics include:
- Approximately 40% of people with AUD also meet criteria for a mood disorder (Hasin et al., 2018, JAMA Psychiatry).
- Adults with PTSD are 2 to 4 times more likely to develop AUD than those without trauma histories.
- Social anxiety disorder has one of the strongest links with AUD, as individuals use alcohol to reduce social inhibition and manage performance anxiety in public settings.
The clinical implication is crucial: treating AUD without addressing the co-occurring mental health condition dramatically increases relapse rates. Integrated treatment approaches that simultaneously target both conditions produce significantly better long-term outcomes.
What Are the Effects of Alcohol Use Disorder?
Alcohol Use Disorder produces three major categories of effects: long-term physical health damage including liver disease, cardiovascular disease, and cancer; neurological and cognitive impairment including memory loss and brain atrophy; and profound social consequences including family breakdown, occupational failure, and legal problems.
The effects of AUD are not limited to the individual; they radiate outward to affect families, workplaces, and communities. The following sections detail how AUD damages the brain over time and erodes social functioning.
What Are the Long-Term Effects of Alcohol Use Disorder on the Brain?
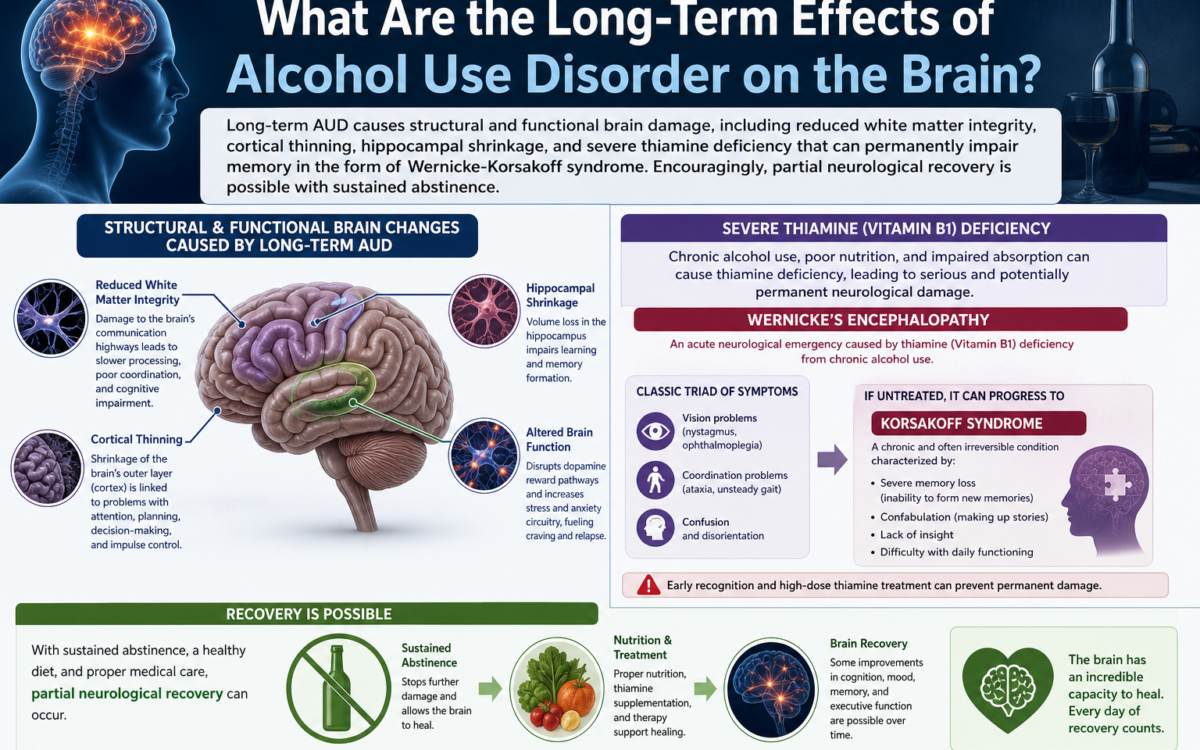
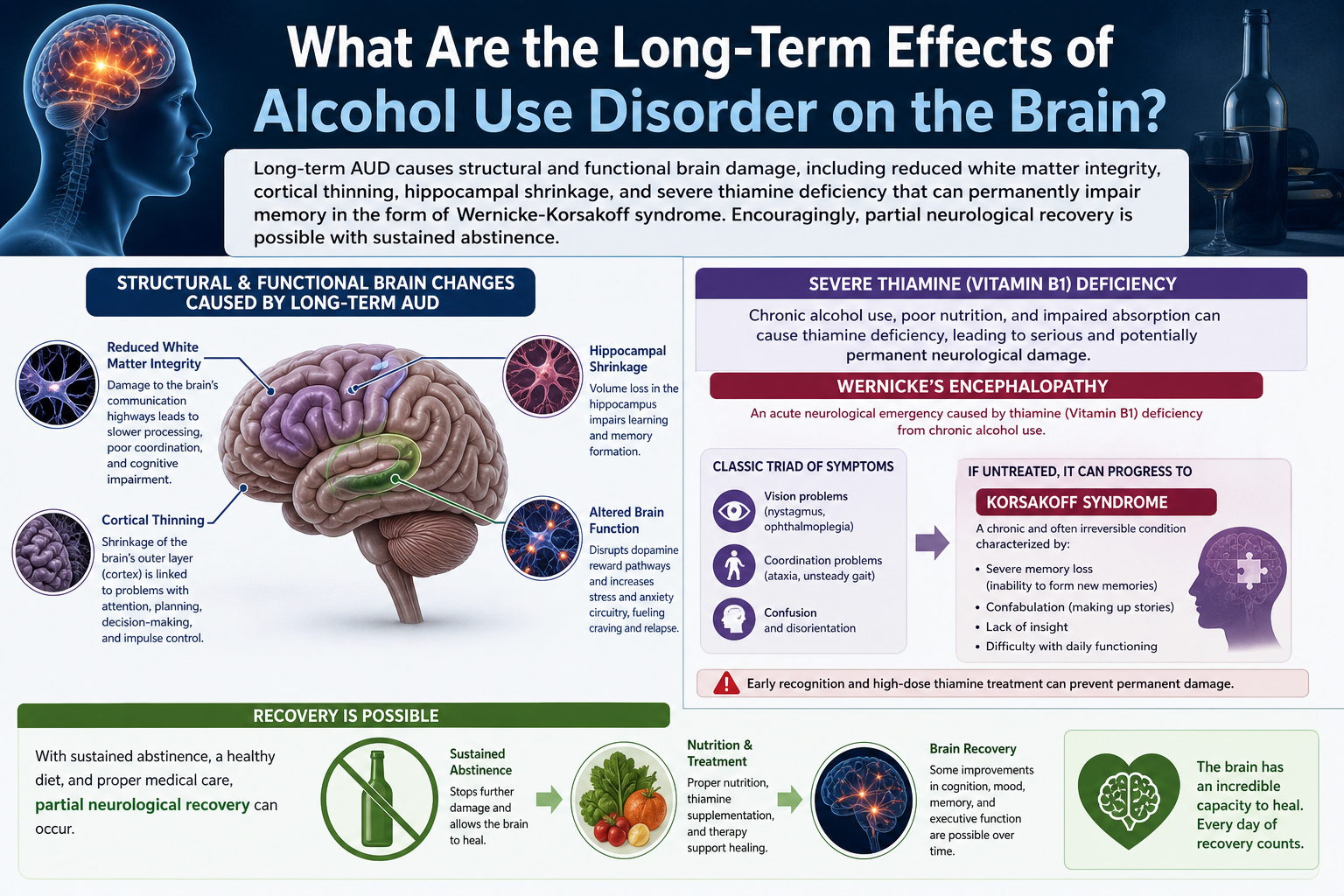
Long-term AUD causes structural and functional brain damage, including reduced white matter integrity, cortical thinning, hippocampal shrinkage, and severe thiamine deficiency that can permanently impair memory in the form of Wernicke-Korsakoff syndrome. Encouragingly, partial neurological recovery is possible with sustained abstinence.
Specific brain-related consequences include:
- Wernicke’s Encephalopathy: An acute neurological emergency caused by thiamine (Vitamin B1) deficiency from chronic alcohol exposure, presenting with confusion, oculomotor dysfunction (eye movement abnormalities), and ataxia. If untreated, it progresses to Korsakoff’s Syndrome.
- Korsakoff’s Syndrome: A chronic amnesic disorder characterized by severe anterograde and retrograde memory impairment, confabulation (unconscious fabrication of memories), and apathy. Up to 80% of people who survive Wernicke’s Encephalopathy develop Korsakoff’s Syndrome.
- Cortical Atrophy: Chronic heavy drinking is associated with measurable reductions in gray matter volume, particularly in the prefrontal cortex, which governs decision-making, impulse control, and judgment. This creates a self-perpetuating cycle: the very brain region needed to choose abstinence is progressively impaired by continued drinking.
- Hippocampal Damage: Alcohol suppresses neurogenesis (the growth of new neurons) in the hippocampus, impairing the formation of new memories and spatial navigation abilities.
According to a study published in Alcoholism: Clinical and Experimental Research (Sullivan & Pfefferbaum, 2019), individuals who maintain sobriety for 6 to 12 months show measurable recovery in white matter integrity and some regional gray matter volume, demonstrating that the brain retains meaningful plasticity even after prolonged alcohol-related damage.
How Does Alcohol Use Disorder Affect Relationships and Social Life?
AUD systematically erodes close relationships and social functioning by creating patterns of broken promises, emotional unavailability, financial strain, and in some cases, alcohol-fueled conflict or neglect. The resulting social isolation then intensifies the psychological distress driving further drinking, creating a self-reinforcing downward spiral.
The specific relational and social consequences include:
- Intimate partnerships: High rates of separation and divorce, sexual dysfunction, domestic conflict, and in some cases, intimate partner violence. Research published in the Journal of Studies on Alcohol and Drugs (Marshal, 2003) found that alcohol involvement is present in 25 to 50% of domestic violence incidents.
- Parenting and child welfare: Children of parents with AUD face elevated risks of emotional neglect, inconsistent discipline, parentification (where children assume adult caretaking roles), and increased likelihood of developing AUD themselves.
- Workplace consequences: Chronic absenteeism, impaired performance, interpersonal conflicts with colleagues, and termination. The CDC estimates that excessive alcohol use cost the U.S. economy $249 billion in 2010, with 72% of those costs attributed to lost workplace productivity.
- Legal consequences: Driving under the influence (DUI) charges, public intoxication, alcohol-related violence, and in severe cases, loss of child custody or professional licensure.
- Social withdrawal: As AUD progresses, many individuals withdraw from friendships, hobbies, and family gatherings that do not involve alcohol, further narrowing their social world and deepening dependence.
What Are the Treatment Options for Alcohol Use Disorder?
Treatment for Alcohol Use Disorder encompasses four main approaches: medically supervised detoxification, pharmacotherapy using FDA-approved medications such as naltrexone, acamprosate, and disulfiram, evidence-based psychotherapy including Cognitive Behavioral Therapy and Motivational Interviewing, and peer support programs such as Alcoholics Anonymous and SMART Recovery.
Treatment is most effective when tailored to the individual’s severity level, co-occurring conditions, and personal circumstances. The following sections address two questions of particular importance to people seeking help: whether AUD can be cured, and which medications are available.
Can Alcohol Use Disorder Be Cured?
No, AUD cannot be “cured” in the traditional sense of complete disease eradication, because it involves lasting changes in brain circuitry that create ongoing vulnerability to relapse. However, AUD is a highly manageable chronic condition, and many people achieve long-term, stable recovery defined by sustained sobriety and restored quality of life.
The clinical community uses the term “recovery” rather than “cure” deliberately. Recovery from AUD is defined by the Substance Abuse and Mental Health Services Administration (SAMHSA) as a process of change through which individuals improve their health and wellness, live self-directed lives, and strive to reach their full potential. This framing acknowledges that recovery is ongoing rather than a single endpoint.
Several important points about the nature of AUD recovery:
- Relapse is common but not failure: Relapse rates for AUD (40 to 60% within the first year of treatment) are comparable to those of other chronic diseases such as hypertension and type 2 diabetes, which also require ongoing management rather than one-time treatment.
- Long-term outcomes improve with treatment engagement: Individuals who participate in a combination of pharmacotherapy and behavioral therapy have significantly better outcomes than those who receive either alone.
- Quality of life can be fully restored: Research consistently shows that people in sustained recovery from AUD report quality of life scores comparable to or exceeding general population norms after several years of sobriety.
According to a national survey by the Recovery Research Institute (2017), an estimated 22.3 million Americans reported being in recovery from a drug or alcohol problem, demonstrating that recovery at scale is achievable.
What Medications Are Used to Treat Alcohol Use Disorder?
Three FDA-approved medications are used to treat AUD: naltrexone, which reduces the rewarding effects of alcohol by blocking opioid receptors; acamprosate, which stabilizes neurochemical imbalances caused by chronic alcohol exposure; and disulfiram, which creates a strongly aversive physical reaction to alcohol consumption.
Each medication works through a distinct mechanism and is appropriate for different clinical situations:
- Naltrexone (brand names: Vivitrol, ReVia): An opioid receptor antagonist that reduces the euphoric and reinforcing effects of alcohol, decreasing both craving and the pleasure derived from drinking. It is available in daily oral form or as a monthly injectable (Vivitrol). Contraindicated in patients taking opioid medications or with acute hepatitis or liver failure. Most effective for individuals who still experience strong urges and pleasure from drinking.
- Acamprosate (brand name: Campral): Works by modulating glutamate and GABA neurotransmission to reduce the hyperexcitability of the nervous system during early abstinence, thereby diminishing protracted withdrawal symptoms such as anxiety, insomnia, and restlessness. Taken as a tablet three times daily. Suitable for patients who have already completed detoxification and are committed to total abstinence. Because it is renally excreted, it is safe for patients with liver disease but contraindicated in severe kidney disease.
- Disulfiram (brand name: Antabuse): Creates a severe aversive reaction (flushing, nausea, vomiting, rapid heartbeat, dyspnea) within minutes of alcohol consumption by blocking acetaldehyde dehydrogenase and allowing toxic acetaldehyde to accumulate. Acts as a behavioral deterrent rather than addressing underlying craving. Requires high patient motivation and is most effective when compliance is supervised by a family member or clinician.
A meta-analysis published in JAMA (Jonas et al., 2014), which reviewed 122 randomized controlled trials involving over 22,000 participants, found that naltrexone was most effective at reducing heavy drinking days, while acamprosate was most effective at supporting abstinence, providing clinicians with clear evidence to guide medication selection based on the patient’s treatment goal.
How Is Alcohol Use Disorder Diagnosed?
Alcohol Use Disorder is diagnosed through a structured clinical evaluation based on 11 DSM-5 criteria, validated screening tools such as the AUDIT and CAGE questionnaire, and supporting laboratory tests including GGT, MCV, and CDT to detect biomarkers of chronic alcohol exposure.
Diagnosis is not a single test but a comprehensive process that combines patient history, standardized assessment, and biological data to establish both the presence and the severity of AUD.
DSM-5 Diagnostic Criteria
The DSM-5 specifies 11 behavioral and physiological criteria for AUD diagnosis. A clinician asks whether, in the past 12 months, the patient has experienced the following:
- Alcohol taken in larger amounts or over a longer period than intended.
- Persistent desire or unsuccessful efforts to cut down or control alcohol use.
- A great deal of time spent obtaining, using, or recovering from alcohol.
- Craving or a strong desire to use alcohol.
- Recurrent alcohol use resulting in failure to fulfill major role obligations.
- Continued alcohol use despite persistent social or interpersonal problems caused by its effects.
- Important social, occupational, or recreational activities given up or reduced because of alcohol use.
- Recurrent alcohol use in physically hazardous situations (e.g., driving).
- Continued use despite knowledge of a persistent physical or psychological problem likely caused or exacerbated by alcohol.
- Tolerance (needing more alcohol to achieve the same effect, or diminished effect with the same amount).
- Withdrawal (characteristic withdrawal syndrome or drinking to relieve or avoid withdrawal symptoms).
Meeting 2 to 3 criteria = Mild AUD. Meeting 4 to 5 = Moderate AUD. Meeting 6 or more = Severe AUD.
Screening Tools Used in Clinical Practice
Beyond the DSM-5 interview, clinicians use validated screening instruments to efficiently identify AUD risk in primary care and general health settings. The three most widely used tools are:
- AUDIT (Alcohol Use Disorders Identification Test): A 10-item questionnaire developed by the WHO, validated across 39 countries, that assesses alcohol consumption frequency, dependence symptoms, and alcohol-related harm over the past 12 months. A score of 8 or above in men and 7 or above in women suggests AUD or hazardous drinking requiring further evaluation.
- CAGE Questionnaire: A rapid 4-item screener that asks about attempts to Cut down drinking, Annoyance at criticism about drinking, Guilt about drinking, and Eye-opener drinks in the morning. Two or more positive responses strongly suggest AUD and warrants comprehensive assessment.
- Laboratory biomarkers: Gamma-glutamyl transferase (GGT) is elevated in approximately 70% of heavy drinkers. Mean corpuscular volume (MCV) is elevated due to alcohol’s toxic effect on red blood cell production. Carbohydrate-deficient transferrin (CDT) is a highly specific marker of chronic heavy alcohol consumption (more than 50g/day for at least 2 weeks) and is particularly useful for monitoring treatment compliance and detecting relapse.
According to the U.S. Preventive Services Task Force (USPSTF, 2018), screening for unhealthy alcohol use in primary care settings for adults 18 and older and providing brief counseling interventions to those who screen positive is a Grade B recommendation, meaning the benefit substantially outweighs the risk and all primary care providers should implement it routinely.
What Are the Withdrawal Symptoms of Alcohol Use Disorder?
Alcohol withdrawal produces a distinct and potentially life-threatening syndrome that includes tremors, diaphoresis (excessive sweating), insomnia, nausea, hypertension, and in severe cases, delirium tremens characterized by seizures, hallucinations, and autonomic instability. Unlike withdrawal from many other substances, alcohol withdrawal carries a significant risk of death without medical supervision.
This supplementary section explores what happens when a person with AUD stops drinking, why abrupt cessation is dangerous, and how clinicians manage the withdrawal process safely.
What Are the Types of Alcoholics?
Researchers at the NIAAA identified 5 subtypes of people with AUD: the Young Adult subtype, the Young Antisocial subtype, the Functional subtype, the Intermediate Familial subtype, and the Chronic Severe subtype. These differ by age of onset, family history, co-occurring disorders, and drinking patterns.
The Young Adult subtype (31.5% of people with AUD) tends to drink less frequently but in binge episodes and rarely seeks treatment. The Functional subtype (19.5%) is typically middle-aged, employed, and high-functioning, often unrecognized by themselves or others. The Chronic Severe subtype (9.2%) has the highest rates of co-occurring psychiatric disorders and the poorest prognosis without intensive intervention. Understanding which subtype a patient belongs to helps clinicians select the most appropriate treatment modality and communication approach.
What Is the Difference Between Alcohol Abuse and Alcohol Addiction?
Alcohol abuse refers to a harmful pattern of drinking causing functional impairment without physical dependence, while alcohol addiction (alcohol dependence) refers to compulsive use with tolerance, withdrawal, and loss of control. The DSM-5 merged both concepts into the single AUD spectrum diagnosis, eliminating the binary distinction.
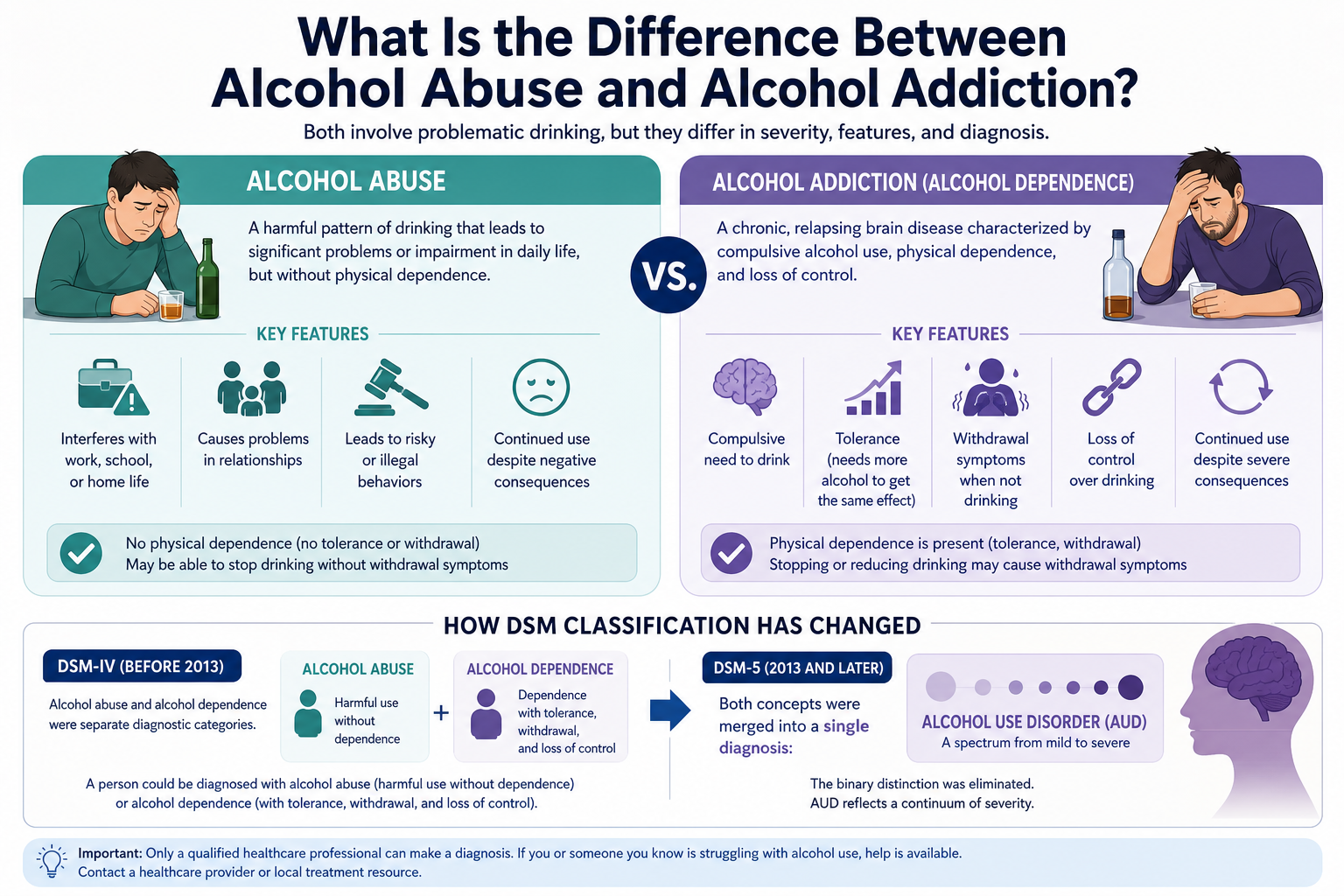
Under DSM-IV, these were separate categories: a person could be diagnosed with alcohol abuse (harmful use without dependence) or alcohol dependence (with tolerance and withdrawal). DSM-5 recognized that this distinction was clinically arbitrary and that both patterns exist on a continuum of severity. The practical implication for patients is that even if someone does not experience physical withdrawal and believes they are “not addicted,” they may still meet DSM-5 criteria for AUD if their drinking is causing measurable harm and they cannot consistently control it. Intervention is warranted as soon as the pattern becomes problematic, not only when physical dependence is established.